The Majority of the Best Scientific Studies Show Masks are Useless, So Why Do People Keep Claiming They Work?
 Foto: dailyveracity.com
Foto: dailyveracity.com
The science is settled on this and has been for a very long time. The vast majority of years of scientific research regarding the efficacy of masks, show they do not prevent the spread of any respiratory illnesses. So why do people keep claiming that they do?
A recent study out of MIT for example concluded that when indoors while wearing a mask, there is no difference if you are six feet away from somebody or sixty feet away. The MIT researchers concluded that this is because the air you exhale is warm air, and warm air will rise. The researchers also say that this is especially true while wearing a mask, as masks push the exhaled air directly upward.
There are many studies just like this one, but the vast majority of the gold standard of scientific research all concludes that masks are completely ineffective at preventing the spread of respiratory illnesses and that healthcare workers wear them just to block big droplets.
A fairly recent study from Denmark involving a sample size of 6,000 participants found that "there was no statistically significant difference between those who wore masks and those who did not when it came to being infected by Covid-19.”
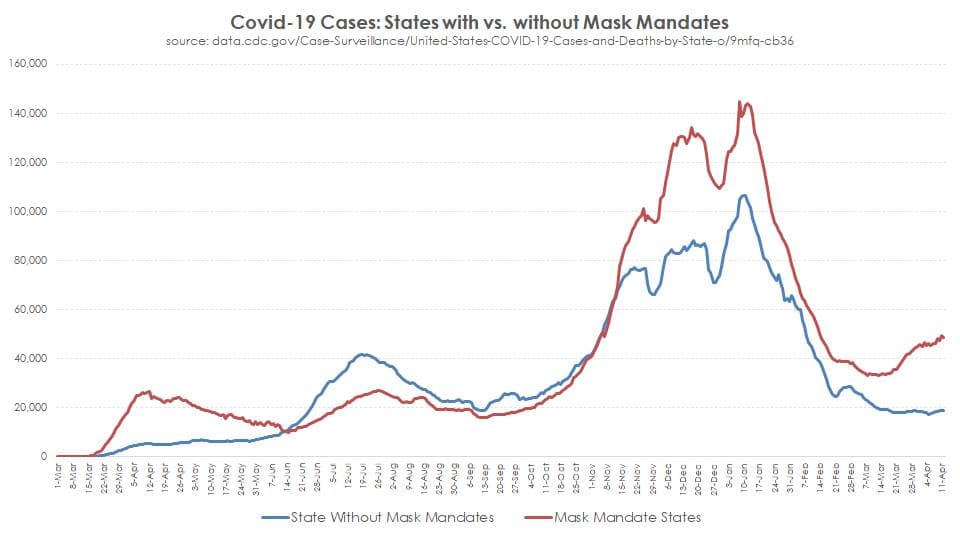
Another ecological study of state mask mandates and their use – which included data from the winter case spike – has found that widespread mask-wearing likely didn’t slow the spread of COVID-19.
The study, conducted by the University of Louisville using data from the Centers for Disease Control and Prevention, found that "80% of US states mandated masks during the COVID-19 pandemic,” but while "mandates induced greater mask compliance, [they] did not predict lower growth rates when community spread was low (minima) or high (maxima).” The study also found that "mask mandates and use are not associated with lower SARS-CoV-2 spread among US states.”
The randomized clinical trial (RCT) is recognized as the most credible research design for clinical investigation. The goal of the RCT is to achieve a valid comparison of the effects of an investigational treatment or treatments with the control treatment (standard of care) in the target patient population. Bias can be reduced by concealing the randomization sequence from the investigators at the time of obtaining consent from potential trial participants. Allocation concealment is a very simple maneuver that can be incorporated in the design of any trial and that can always be implemented.
This means that the only way to remove bias from scientific research in the medical field is with randomized clinical trials. Contrary to popular belief, every single RCT ever performed on mask usage and prevention of infection for laboratory-confirmed influenza, the common cold, or other respiratory viruses shows that masks are ineffective.
There is a sum total of zero randomized clinical trials showing that masks prevent any of the aforementioned illnesses. As you read through the following trial summaries and their conclusions, recall the damage we have already knowingly inflicted upon the population, and the health risks of the shutdowns that we have already consciously accepted in our quest to "trust the science.”
Jacobs, J. L. et al. (2009) "Use of surgical face masks to reduce the incidence of the common cold among health care workers in Japan: A randomized controlled trial,” American Journal of Infection Control, Volume 37, Issue 5, 417–419.
N95-masked health-care workers (HCW) were significantly more likely to experience headaches. Face mask use in HCW was not demonstrated to provide benefit in terms of cold symptoms or getting colds.
Radonovich, L.J. et al. (2019) "N95 Respirators vs Medical Masks for Preventing Influenza Among Health Care Personnel: A Randomized Clinical Trial,” JAMA. 2019; 322(9): 824–833.
"Among 2862 randomized participants, 2371 completed the study and accounted for 5180 HCW-seasons. … Among outpatient health care personnel, N95 respirators vs medical masks as worn by participants in this trial resulted in no significant difference in the incidence of laboratory-confirmed influenza.”
Long, Y. et al. (2020) "Effectiveness of N95 respirators versus surgical masks against influenza: A systematic review and meta-analysis,” J Evid Based Med. 2020; 1–9.
"A total of six RCTs involving 9,171 participants were included. There were no statistically significant differences in preventing laboratory-confirmed influenza, laboratory-confirmed respiratory viral infections, laboratory-confirmed respiratory infection, and influenza-like illness using N95 respirators and surgical masks. Meta-analysis indicated a protective effect of N95 respirators against laboratory-confirmed bacterial colonization (RR = 0.58, 95% CI 0.43-0.78). The use of N95 respirators compared with surgical masks is not associated with a lower risk of laboratory-confirmed influenza.”
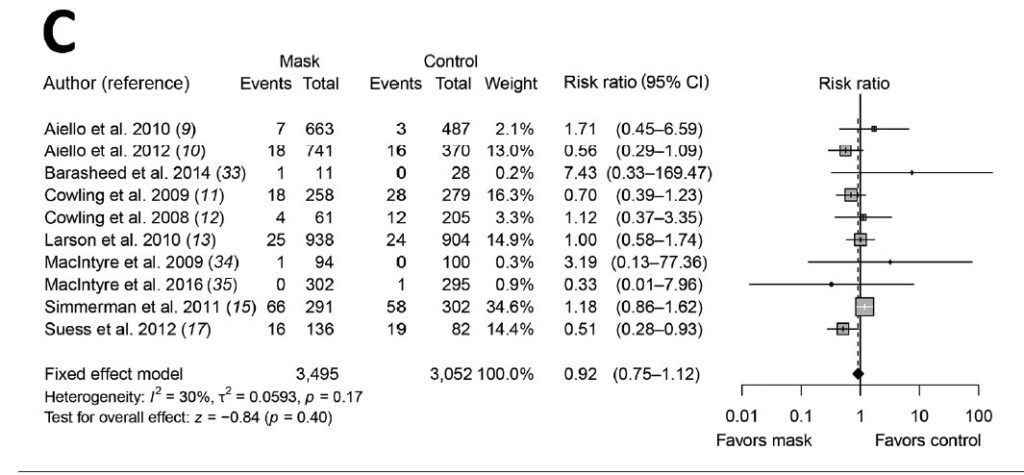
Cowling, B. et al. (2010) "Face masks to prevent transmission of influenza virus: A systematic review,” Epidemiology and Infection, 138(4), 449-456.
None of the studies reviewed showed a benefit from wearing a mask, in either HCW or community members in households (H). See summary Tables 1 and 2 therein.
Bin-Reza et al. (2012) "The use of masks and respirators to prevent transmission of influenza: a systematic review of the scientific evidence,” Influenza and Other Respiratory Viruses 6(4), 257–267.
"There were 17 eligible studies. … None of the studies established a conclusive relationship between mask/respirator use and protection against influenza infection.”
Smith, J.D. et al. (2016) "Effectiveness of N95 respirators versus surgical masks in protecting health care workers from acute respiratory infection: a systematic review and meta-analysis,” CMAJ Mar 2016
"We identified six clinical studies … . In the meta-analysis of the clinical studies, we found no significant difference between N95 respirators and surgical masks in associated risk of (a) laboratory-confirmed respiratory infection, (b) influenza-like illness, or (c) reported work-place absenteeism.”
Offeddu, V. et al. (2017) "Effectiveness of Masks and Respirators Against Respiratory Infections in Healthcare Workers: A Systematic Review and Meta-Analysis,” Clinical Infectious Diseases, Volume 65, Issue 11, 1 December 2017, pages 1934–1942,
"Self-reported assessment of clinical outcomes was prone to bias. Evidence of a protective effect of masks or respirators against verified respiratory infection (VRI) was not statistically significant.”
President Joe Biden criticized the governors of Texas and Mississippi for lifting their mask mandates, calling the decision "Neanderthal thinking.”
"The last thing, the last thing we need is Neanderthal thinking that in the meantime, everything’s fine, take off your mask, forget it,” Biden commented.
Prior to his statement, White House press secretary Jen Psaki also criticized governors for lifting mask mandates.
"The entire country has paid the price for political leaders who ignored the science when it comes to the pandemic,” she said.
Despite the criticism, coronavirus cases fell in Texas more than two weeks after Abbott lifted the restrictions, and even further weeks after that.
The science on masks preventing the spread of viruses has been settled for years, and this is why you saw the opposite of what was predicted in Texas occur. The virus is seasonal – just as influenza is – and rises and falls with the levels of vitamin d in the population.
Some studies have found that vitamin D levels increase in summer and decrease in winter due to dependency of vitamin D on sunlight. Studies have also shown that this seasonal variation might depend on latitude, since it has been found that vitamin D production is greater on latitudes close to the equator.
Email exchanges between Dr. Anthony Fauci and other scientists, including the President of the EcoHealth Alliance – a group that has extensive ties to the Wuhan lab gain of function research – were discovered in a trove of emails obtained by The Washington Post through a FOIA request.
Included in the emails is Dr. Fauci’s response to the former health and human services secretary, Sylvia Burwell, when she asked him about wearing face masks while traveling.
"Masks are really for infected people to prevent them from spreading infection to people who are not infected rather than protecting uninfected people from acquiring infection. The typical mask you buy in the drug store is not really effective in keeping out virus, which is small enough to pass through material. It might, however, provide some slight benefit in keep out gross droplets if someone coughs or sneezes on you,” Fauci wrote in a response.
The emails also reveal that Dr Fauci was informed at the end of March about pooled randomized, controlled trial data showing masks did not work in community settings to prevent the spread of respiratory viral infections.
As we know, most Americans are reusing their masks repeatedly. Many Americans store them on their rear-view mirrors, in their pockets, and even on the table that they’re eating on at restaurants.
This can not be sanitary or healthy by any metric, and some studies suggest there is a great risk for microbial pathogen infections from constantly reusing masks.
One research focus area that appears to be entirely lacking, in examining the harms of masks, is the broad psychological impact of mandatory masking policies applied to the general population.
Some studies have found wide-ranging negative psychological impacts on forced mask usage, especially among children.
The research is lacking now, but some researchers suggest we will find that the negative effects of forced mask usage could include chronic stress, fear, anxiety, the activation of the ‘fight of flight’ response, to even causing skin conditions and maybe even cancer from the micro-plastics most medical masks contain.
Source: The Daily Veracity
Covid-19 infections commonly occur via aerosolized particles, not just droplets. Masks and air filters can remove very small particles, such as bacteria and viruses but a single coronavirus particle size ranges from 70–90 nm. This is one hundred times smaller than a tenth of a micron.
The renowned UK science journal, The Lancet published a paper concluding that "Small aerosol particles smaller than 5 μm in aerodynamic size are most likely to remain” following filtering of the air.
A brand new N-95 mask – which is not what most of the population uses – only filters out particulate matter larger than .3 microns.
ActiveNews nu a primit niciodată altă publicitate decât cea automată, de tip Google, din care o îndepărtăm pe cea imorală. Aceasta însă nu ne asigură toate costurile.
Ziarele incomode sunt sabotate de Sistem. Presa din România primeste publicitate (adică BANI) doar în măsura în care este parte a Sistemului sau/și a Rețelei Soros. Sau dacă se supune, TACE sau MINTE.
ActiveNews NU vrea să se supună. ActiveNews NU vrea să tacă. ActiveNews NU vrea să mintă. ActiveNews VREA să rămână exclusiv în slujba Adevărului și a cititorilor.
De aceea, are nevoie de cititorii săi pentru a supraviețui așa cum este acum. Dacă și tu crezi în ceea ce credem noi, te rugăm să ne sprijini să luptăm în continuare pentru Adevăr, pentru România!
RO02BTRLRONCRT0563030301 (lei) | RO49BTRLEURCRT0563030301 (euro)
Pe același subiect

Viganò: Conclavul este falsificat – De aceea, viitorul Papă nu va avea autoritate

Peninsula Iberică este noul Wuhan?

A vrut un Nürnberg al Covidismului: A fost aruncat în pușcărie!

BTI: A venit adevărata nucleară: ambasada SUA sugerează că alegerile nu vor fi recunoscute

EMISIUNE LIVE: Doru Paraschiv, ofițerul de informații care l-a prins cu minciuna pe Marian Enache de la CCR ÎN DIRECT la ActiveNews și Starea de Libertate. ACTUALIZARE

Visul umed al Europei e mai aproape ca oricând de a deveni realitate: Să se spele pe cap cu Războiul și cu Zelenski!
Recomandările noastre



22 aprilie 1990, startul Pieței Universității. În urmă cu 35 de ani începea cea mai amplă manifestație anticomunistă din Europa Centrală și de Est. VIDEO și GALERIE FOTO

Autentifică-te sau înregistrează-te pentru a trimite comentarii.
Comentarii (2)